Paul Manley Back Pain and RSI Clinic
Paul Manley, M.A.O.(Manip), Registered OsteomyologistFor muscle and joint problems

RSM (Royal Society of Medicine)
Specialist in the treatment of Musculo-skeletal problems
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line
19/01/2026
The physiological basis for Enhanced Cranial technique.
The brain pulsates as we breath and with our heartbeat.
This makes the cerebro-spinal fluid flow and mix throughout our central nervous system.Thus when we increase our heart rate it 'clears' our head.
The movie below was created using the most advanced MRI real-time tomography thus far and this amplified view shows vividly the interaction of the heartbeat as it pumps the circulation of the blood and cerebro-spinal fluid (CSF) throughout the brain.
The brain shrinks during sleep up to 20%.
Reference:"Ah, to sleep, perchance … to shrink your neural connections? That's the conclusion of new research that examined subtle changes in the brain during sleep.
The researchers found that sleep provides a time when the brain's synapses — the connections among neurons—shrink back by nearly 20 percent. During this time, the synapses rest and prepare for the next day, when they will grow stronger while receiving new input—that is, learning new things, the researchers said.
Without this reset, known as "synaptic homeostasis," synapses could become overloaded and burned out, like an electrical outlet with too many appliances plugged in to it, the scientists said."
Why do we yawn when we are falling asleep and when we are waking up?
The effect of yawning is to 'squeeze' the brain due to the increase in venous pressure. This promotes the appropriate state of waking or sleeping as required.
Whilst we sleep there is a steady flow of circulation which enables the brain to excrete the metabolites that build up during the day. Our thoughts and experiences of the day leave behind many neuro-chemicals which must be excreted.
The more we learn during the day, the more there is to remove at night. Hence children sleep much more than older people. In fact as we get much older we sleep much less. This can lead to confusion and down the path to senility.
Enhanced Cranial Techniques (ECM)
1. The bony component.
This component looks at the growth of the cranium. It takes into account asymmetries of the cranium. Fixations of the sutures of the skull are a normal result of trauma be it from birth or acquired through trauma during infancy and in adulthood.
2. The elastic component.
This is the factor which determines the 'elasticity' of the sutures. When the elastic co-efficient is low the pressures passing through the cerebro-spinal fluid rises with a spectrum of negative effects on the circulation of the brain. This is measured through evaluation of the 'pulsatility index'.
3. The fluid component.
The cerebro-spinal fluid which circulates throughout the brain should not exceed a specific pressure. Its production in the center of the brain unfortunately will continue despite the pressure leading to compromise of the brain stem functions. At its extreme such a rise will result in coma and ultimatley death. At its minimum it can affect the brain stem activation system resulting in a wide range of symptoms. In adults it can manifest as mood changes, fuzziness and lack of concentration. Whilst in infants it can result in poor learning and concentration levels.
4. The neuro-physiological component.
Because the rise in pulsatility index affects the brain stem regulatory systems factors such as blood pressure, digestion, heart rate, autonomic vervous system aberrations, panic attacks and a potentially psychological and psychiatric conditions. See more on the Headway website linked below: In extremis it can result in personality changes and psychoses. Concussion can cause the most extreme of such symptoms (read here for a full list)
My specialised techniques aim to manually loosen or soften the sutures of the vault bones of the cranium thereby acieving a reduction in the pulsatility index.
As we grow older we can acquire various head injuries which can result in compression and fixation of the cranial sutures:
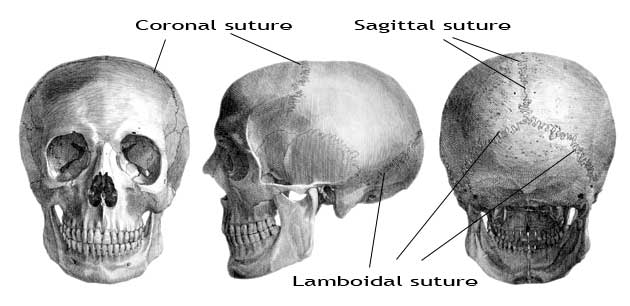
Figure 1
The sutures of the vault bones of the human cranium.
The cranium has a certain degree of elasticity. this is called the 'elastance co-efficient'. When this is compromised symptoms can follow.
ECM is applied to the cranium in oreder to 'soften' the sutures thus creating greater elastance.
Following some years of intensive study of the cranium I concluded that a fairly simple approach to achieving greater elastance was possible. The principle is simple and consists of expanding the skull upwards by raising the parietal bones, loosening the coronal suture and expanding the lambdoidal sutures.
Cranial Osteopathy and Sacro-cranial technique are dubious as commonly practiced.
The most commonly used approach entitled 'Cranial technique' or 'Sacro-cranial' technique applied by practitioners whilst restful in result is entirely missing the point in my opinion. That point being to learn how to apply manipulative techniques to the cranium which effectively increase the elasticity. Their 'functional' approach as invented by Mr. John Upledger is 'poppycock' and evidence of 'wishy' thinking. The cabal of its adherents would be much more effective if only they knew more about ECM.However, with babies and children such 'gentle'techniques can sometimes be effective but depend to a large degree on both the gullibility of the parents and the practitioners so indoctrinated.
The following
is an abridged version of an article published by Bastyr
University, Journal of Naturopathic Medicine ( Oregon ),
The New Zealand Journal of Osteopathy and by Temple University
(Philadelphia), Frontier Perspectives, all 1993-1995. Author: Paul Manley D.O. (ESO 1980)
In one way this short
paper describes mechanisms by which infants may suffer
in the short and the long term from cranial abormalities,
in another, it alludes to methods of diagnosis and manual
treatment which can provide relief from such problems.
Enhanced Cranial Manipulation (ECM) is a 'nuts and bolts' approach to cranial problems and represents a unique collection of manipulative techniques as applied to the cranium. This is in contrast to the esoteric approach fostered by the ubiquitous practitioners of Cranio-sacral therapy etc..
The object of ECM is to optimize the elastance co-efficient of the cranium. This is acheived via manual de-compression techniques applied directly to the cranium. Stimulation of the venous drainage by increasing the circulation of the scalp is also a beneficial by-product of treatment.
The techniques are appropriate for cranial and autonomic symptoms only. They are not used for fixing a 'low-back pain' for example, other, more efficient, traditional techniques can deal with such problems.
The following points must be considered when forming an understanding of the cranium in relation to its contents:
1. The cerebral capsule (bone and membrane) changes in degrees of resilience due to the changes in ICP therein. The vault bones only grow in response to internal expansive pressures as the brain grows.
2. Intra-cranial pressure ( ICP ) varies in response to the following:
a. The rate of cerebro-spinal fluid ( CSF ) production.
b. The rate of CSF drainage.
c. The elasticity of the cerebral capsule.
d. The degree of responsiveness of the neurohumoral mechanisms which react with ICP fluctuations.
3. Increased ICP, even of short duration, can compromise cerebral circulation especially in the region of the brain stem activational and regulatory areas.
4. The "elastic coefficient" or elasticity of the cerebral capsule exerts a damping or shock absorbing action on ICP variations, thus providing a buffer between the CSF and the CNS.
5. The
lower the elasticity of the cranium, the higher the ICP rises.
Infant development of the cranium:
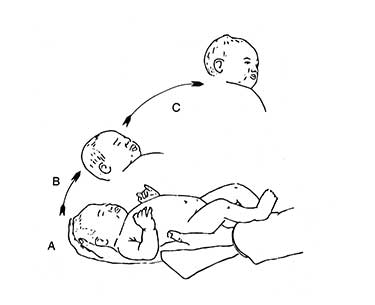
During the passage of the infant through the birth canal, the head deforms, causing overlap of the coronal, sagittal and lambdoidal sutures.
This overlapping usually disappears during the first three days of life. It is most pronounced in premature infants due to the wideness of the sutures but nonetheless appears consistently in the normal neonate.
|
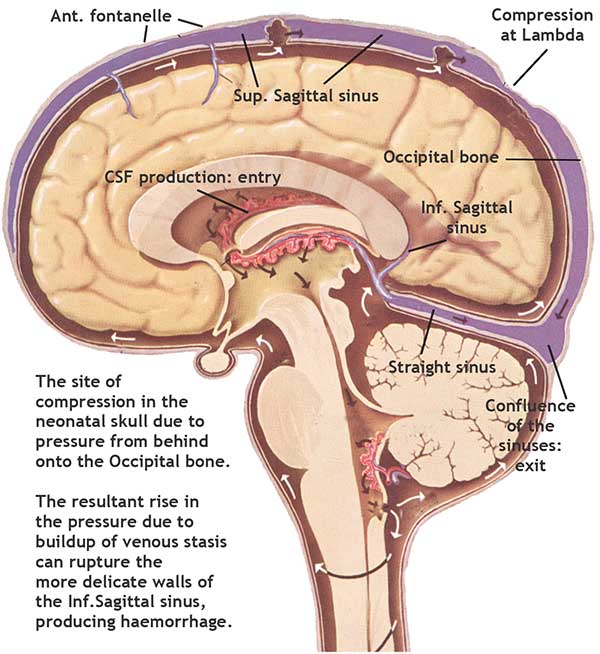
Figure
2 Compression of the Superior Sagittal sinus due to external pressure on the Occipital bone |
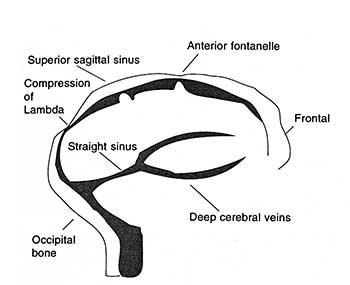
Lambdoidal overlap and superior sagittal sinus ( SSS ) compression may be produced merely by laying the infant on its back, head resting on its occipital bone. The pressure on the occipital bone effectively blocks the SSS. The overlap is accentuated when the infant is supine for prolonged periods. The compression of the SSS produces slowing in the cerebral circulation time and diverts drainage into the deep venous system. Due to the thinness of these vein walls at this age, intracerebral hemorrhage can occur and is one of the major causes of death in infants, especially preterm.
The
practitioner should be capable of adequately differentiating between
potential contributary factors.
Craniosynostosis is a term which
applies to the types of deformity affecting the shape and elastic
function of the skull resulting from the premature closure of one
or more sutures. This can occur in response to direct trauma such
as forceps delivery, constant moulding pressures such as sleeping
on the same side of the head, or from congenital or genetic origins.
Growth responses to premature suture closure.
Figure 3 Growth responses to premature suture closure |
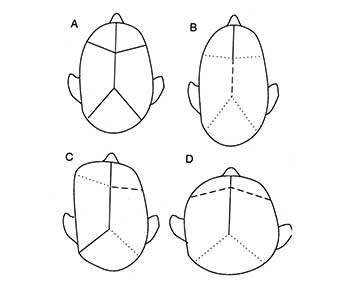
Figure 3: Legend
Solid
line ____ normal
Dotted line ..... premature
closure
Dashed line - - - secondary compensation
(expansion)
A:
Normal
B: Sagittal synostosis
C: Unilateral coronal closure
D: Bilateral coronal closure
Figure 3 illustrates the various configurations most likely to occur. The synostotic patterns can persist into adulthood and may result in gross deformity or in sutural fixations. The incidence of mental and/or motor deficit is high with this pathology. This is due to the effect on the ICP either by hampering drainage of CSF or by decreased elasticity failing to allow for optimal ICP fluctuations. Palpation of Lambda (the junction of the parietal and occipital bones) in order to ascertain the prescence of overlap is very important. Ridging of the sagittal and frontal sutures is generally present and palpable in premature closure, even into adulthood.
|
The shape of the anterior fontanelle (Figure 4 ), whilst still patent (un-ossified), can be very revealing with regard to the ICP. Normally the ICP is increased (from atmospheric pressure as baseline) when the infant is in the horizontal position and the fontanelle shows as convex, whereas in the vertical position the ICP is normally subatmospheric and the fontanelle will be concave. Thus, when the ICP is raised and the infant is in the vertical position the fontanelle will be convex, i.e. a bump.
There are a few exceptional circumstances when this principle does not apply and in such cases the fontanelle remains flat. This maneuver can be used to determine whether the ICP is in the normal range when used as a part of the usual diagnostic procedures.
When assessing the appropriateness of treatment, aggravating factors, and prognosis, the following factors must be considered:
1. ICP
increases instantly with crying, laughing, abnormal respiratory
patterns, abdominal straining, agitation, increase intrathoracic
pressure, raised central venous pressure and pain.
2. The pressure of encircling bands and constrictions to the
neck can produce ICP rise, the bands of nasal cannulae, phototherapy
patches, tight collars, etc.
Because ICP rise alters the ratios of the monoamine axis (5HT, noradrenaline and dopamine) in the brain stem activational systems, general symptoms are many and vary greatly in both type and severity.
The most obvious signs and symptoms are:
1. Sensorimotor
and mental deprecation (i.e. listlessness, sleeplessness
or lack of normal responsiveness, difficulty suckling, gripey
and agitated).
In the adult, agitation, emotional volatility, personality changes, headaches, inability to concentrate, drowsiness can all be symptoms of the need to improve the elastic compliance of the cranium.
2. Apneic (cessation of breathing) attacks and convulsions.
3. Neurological deterioration indicative of severe brain stem compression (such as inability to perform ocular tracking or lack of standard reflexes).
Even lesser degrees of ICP derangement can, over time, fundamentally disrupt and cause delay to the sequences involved in the laying down of the vital CNS developmental programs. This maturing and myelinatiing process is the basis for maximal motor and cognitive development in all infants. Indications of severe ICP compression must be assessed by a pediatric neurologist before initiation of any treatment.
References:
1. Compression
of the superior sagittal sinus by neonatal calvarial moulding.
Radiology. 1975;(115): 6359
2. Changes in Superior Sagittal Sinus Blood Velocities Due to Postural Alterations and Pressure on the Head of the Newborn Infant
Cowan, et al. Pediatrics 1985; 75:6 1038-1047
3. Intracranial pressure and obstructive sleep apnea. Chest,
1989 (95)2: 27983
4. Degeneration of neurons in the thalamic reticular nucleus
following transient ischemia due to raised intracranial
pressure: Excitogenic degeneration mediated via non NMDA receptors.
Brain Research 1989; (501): 12943
5. Cerebrospinal fluid pulse waveform as an indicator of
cerebral autoregulation. J. Neurosurgery 1982 (56):6668
6. Intracranial compliance is time dependant. J. Neurosurgery
1987 20(3) :38995
7. A fast method of estimating the elasticity of the intracranial
system. J. Neurosurgery 1977; (47): 1926
07925 616 753
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line