Paul Manley Back Pain and RSI Clinic
Paul Manley, M.A.O.(Manip), Registered OsteomyologistFor muscle and joint problems

RSM (Royal Society of Medicine)
Specialist in the treatment of Musculo-skeletal problems
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line
19/01/2026
The Diaphragm
The central tendon of the diaphragm is a thin but strong aponeurosis situated near the center of the vault formed by the muscle, but somewhat closer to the front than to the back of the thorax, so that the posterior muscular fibers are longer. It is situated immediately below the pericardium, with which it is partially blended.
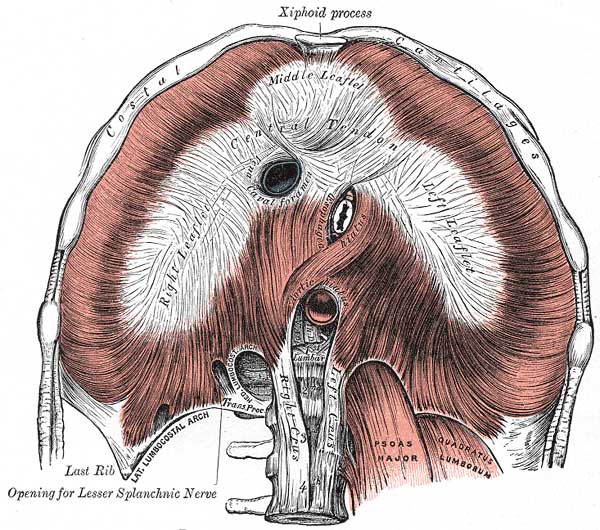
Anterior view of diaphragm showing its lines of application
where it attaches to the ribs and to the central tendon.
The shape of the diaphragm.
It is shaped somewhat like a trefoil leaf, consisting of three divisions
or leaflets separated from one another by slight indentations. The
right leaflet is the largest, the middle, directed toward the xiphoid
process, the next in size, and the left the smallest. In structure
the tendon is composed of several planes of fibers, which intersect
one another at various angles and unite into straight or curved bundles—an
arrangement which gives it additional strength.
During inspiration the diaphragm contracts causing the central tendon
to be drawn downwards which partially flattens the domes. The result
is an enlargement of thoracic cavity and reduction in intra-thoracic
pressure.
Physiologically this means that air enters the lungs and venous return
to the heart is enhanced. During inspiration the central tendon retains
its shape due to its tendonous nature and prevents constriction of
the inferior vena cava or aorta, however the oesophagus is surrounded
by muscle at the oesophageal hiatus and is constricted (food is difficult
to swallow with inspiration).
The crura of the diaphragm.
At their origins
the crura are tendinous in structure, and blend with the anterior
longitudinal ligament of the vertebral column.
The right crus, larger and longer than the left, arises from the anterior
surfaces of the bodies and intervertebral fibrocartilages of the upper
three lumbar vertebrae. The left crus arises from the corresponding
parts of the upper two lumbar vertebrae only. The medial tendinous
margins of the crura pass anteriorly and medialward, and meet in the
middle line to form an arch across the front of the aorta known as
the median arcuate ligament; this arch is often poorly defined. The
area behind this arch is known as the aortic hiatus. From this series
of origins the fibers of the diaphragm converge to be inserted into
the central tendon.
The fibers arising from the xiphoid process are very short, and occasionally
aponeurotic; those from the medial and lateral lumbocostal arches,
and more especially those from the ribs and their cartilages, are longer,
and describe marked curves as they ascend and converge to their insertion.
The fibers of the crura diverge as they ascend, the most lateral being
directed upward and lateralward to the central tendon. The medial fibers
of the right crus ascend on the left side of the esophageal hiatus,
and occasionally a fasciculus of the left crus crosses the aorta and
runs obliquely through the fibers of the right crus toward the vena
caval foramen.
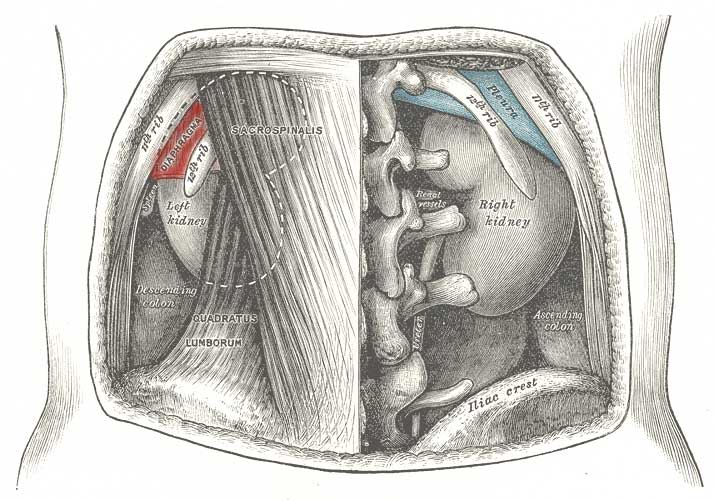
Rear
view of torso showing location of diaphragm
( in red ) and
its relation to the kidneys and rear of the ribcage.
Atmospheric
pressure.
Breathing consists of inspiration (air flow into lungs) and expiration
(air flow out of lungs). Atmospheric pressure at sea level is 760 mm
Hg. The intrapulmonary pressure within the alveoli of the lungs always
equalizes itself with the atmospheric pressure outside the body. The
pressure within the pleural cavity (intrapleural pressure) also fluctuates
with breathing phases. However, the intrapleural pressure is always
4 mm Hg less than the pressure in the alveoli, so it is said to be
negative relative to both the intrapulmonary and atmospheric pressures.
Inspiration
Contraction
of the diaphragm causes the volume of the thoracic cavity to enlarge.
This temporarily decreases the gas pressure within the lungs. Air
rushes in to equalize the intrapulmonary pressure with atmospheric
pressure.
Inspiration depends on the action of the diaphragm.
Expiration
Quiet expiration is a passive
process that just depends on the natural elasticity of the lungs.
Thus the pressure in the lungs is temporarily increased as the
tissue recoils, causing gas to flow out of the lungs. Forced
expiration uses abdominal wall muscles.
07925 616 753
Location: 8-10 Boston Place, Marylebone, London NW1 6QH
Next to Marylebone Station, Main line trains and Bakerloo line